Sinan Mohammed Abdullah AL-Mahmood1 ![]() ,
Shahrin Tarmizi Bin Che Abdullah2,
Nik Nur Fatnoon Nik Ahmad2,
Abdul Hadi Bin Mohamed2,
Tariq Abdul Razak2
,
Shahrin Tarmizi Bin Che Abdullah2,
Nik Nur Fatnoon Nik Ahmad2,
Abdul Hadi Bin Mohamed2,
Tariq Abdul Razak2
For correspondence:- Sinan AL-Mahmood Email: sinanmohamed@iium.edu.my Tel:+601111002473
Received: 20 January 2016 Accepted: 9 May 2016 Published: 28 June 2016
Citation: AL-Mahmood SM, Che Abdullah ST, Ahmad NN, Mohamed AH, Razak TA. Analgesic synergism of gabapentin and carbamazepine in rat model of diabetic neuropathic pain. Trop J Pharm Res 2016; 15(6):1191-1195 doi: 10.4314/tjpr.v15i6.11
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate synergy in the analgesic effects of a combination therapy of carbamazepine (CBZ) and gabapentin (GBP) in diabetic neuropathic pain.
Methods: Neuropathic pain was produced in rats by a single intraperitoneal injection of streptozotocin (STZ) at 60 mg/kg. CBZ, GBP, and their combination were orally administered at varying doses (GBP 30 - 180 mg/kg; CBZ 20 - 40 mg/kg) comparable to their therapeutic doses in humans. Nociceptive responses in the diabetic rats were assessed using hot plate test.
Results: Hot plate latency significantly increased with oral administration of GBP at a dose of 180 mg/kg when compared with control group (p < 0.05), while at a dose of 90 mg/kg, the increase was not significant. Oral administration of CBZ at doses of 20 and 40 mg/kg did not produce any significant impact on hot plate latency. However, a combination of GBP at 90 mg/kg and CBZ at 20 mg/kg produced significant increase in latency, compared with control group and other groups (p < 0.05), except the group that received 180 mg/kg GBP. The combination of low dose GBP 30 mg/kg and carbamazepine 30 mg/kg had no significant effect on latency (p > 0.05).
Conclusion: The results obtained in this study provide useful information on the combination therapy of GBP and CBZ, which may be applied in the treatment of pain in diabetic neuropathy.
Introduction
Diabetic neuropathy is a common and costly complication of both types of diabetes (I and II). The prevalence of neuropathy is about 8 % in newly diagnosed patients and greater than half of patients with long-standing diabetes [1]. Increasing evidence suggest that pre-diabetic conditions are also associated with some forms of neuropathy [2]. An estimated 15 % of all patients with diabetes will develop foot ulcers; diabetic neuropathy is the leading cause of non-traumatic limb amputation [3].
A variety of anticonvulsants and local anaesthetic drugs suppress abnormal discharge originating at nerve injury sites and associated dorsal root ganglions (DRGs) via sodium channel blockage. These include CBZ, phenytoin, tocainide, and lidocaine [4]. CBZ is the first antiepileptic drug utilized in many clinical trials and has been used for long to manage diabetic neuropathy pain [5]. Earlier studies recommended that CBZ might be effective in diabetic neuropathy and, in France; CBZ is endorsed for treating neuropathic pain in adults. The normal therapeutic dose of CBZ is between 600 and 1600 mg/day, initially at 200 mg/day, which is gradually increased every three days by 200 mg/day, depending on the unwanted effects and response [6]. CBZ appears to limit the repetitive firing of action potentials evoked by a sustained depolarization by slowing down the rate of recovery of voltage-activated Na+ channels [7].
GBP is an anticonvulsant drug with an established outcome against diabetic neuropathic pain [8]. It was used for many years in the treatment of partial epilepsy and was the approved medication for neuropathic pain in the UK. It is well accepted and appears to be effective at a daily dose of 1800 mg. GBP, a synthetic analogue of the neurotransmitter Ɣ-aminobutyric acid (GABA) does not interact specifically with GABA receptors but rather modulates the activity of high-threshold calcium channels, and is successful in relieving indices of allodynia and hyperalgesia in animal models [9]. Moreover, GBP has mild side effects profile. In view of the consequences of these qualities, GBP ought to be considered a first‐line treatment for neuropathic pain. Evidence of the adequacy of anticonvulsant medications in the treatment of neuropathic pain are on the increase, and have been clearly demonstrated with GBP and CBZ [10].
Combination therapy is an effective strategy in neuropathy treatment, where a reduction of dose could decrease unpleasant side effects while producing effective analgesic outcomes. This study was carried out to investigate the effectiveness of GBP and CBZ combination therapy in the management of diabetic neuropathy pain in a rat model.
Methods
Experimental animals
Seventy adult female Sprague-Dawley rats weighing between 225 and 250 g were used. All animals were housed in groups of 2 - 3 at a temperature 22 ± 1 ºC and relative humidity of 60 – 70 %, in a room with a 12:12 h light/dark cycle. The animals were allowed free access to water and normal diet. All experimental protocols involving animals and their care were approved (ref. no. IACUC-IIUM/2015-6-34) by the institutional animal care and used committee of International Islamic University Malaysia, and the experimental protocols followed the “Guide for the care and use of laboratory animals” [11].
Induction of diabetes
STZ (Merck) was dissolved in 0.1 M Citrate Buffer at pH 4.5 immediately before intraperitoneally (i.p) injection. To induce diabetes, rats received a single i.p. injection of STZ (60 mg/kg body weight) following an overnight fast. Hyperglycaemia was confirmed three days later by the measurement of tail-vein blood-glucose concentration in fasting rats. Only animals with a blood glucose of 15 mmol/L or above were considered diabetic and used for the experiments.
Drug administration
Gabapentin (Neurontin, Pfizer, USA) was suspended in 0.9 % saline and administered three times daily. Liquid Carbamazepine (Novartis, Switzerland) was administered once daily; all drugs were administered to rats by oral gavage.
Experimental design
The rats were divided into seven groups of ten animals.
Group I: Diabetic (STZ) + GBP 180 mg/kg: Animals received oral gavage of GBP (180 mg/kg) daily for 1 week after four weeks of diabetes induction.
Group II: Diabetic (STZ) +GBP 90 mg/kg: Animals received oral gavage of GBP (90 mg/kg) daily for 1 week after four weeks of diabetes induction.
Group III: Diabetic (STZ) +CBZ 40 mg/kg: Animals received oral gavage of CBZ (40 mg/kg) daily for 1 week after four weeks of diabetes induction.
Group IV: Diabetic (STZ) +CBZ 20 mg/kg: Animals received oral gavage of CBZ (20 mg/kg) daily for 1 week after four weeks of diabetes induction.
Group V: Diabetic (STZ) + (GBP 90 mg/kg+ CBZ 20 mg/kg): Animals received oral gavage of GBP 90 mg/kg+ CBZ 20 mg/kg daily for 1 week after four weeks of diabetes induction.
Group VI: Diabetic (STZ) + (GBP 30 mg/kg+ CBZ 40 mg/kg): Animals received oral gavage of GBP 30 mg/kg+ CBZ 40 mg/kg daily for 1 week after four weeks of diabetes induction.
Group VII: Diabetic (STZ) Control: Animals received oral gavage of 0.9 % saline daily for 1 week after four weeks of diabetes induction.
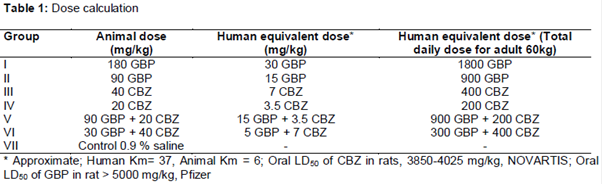
Dose calculation
All doses were calculated by using the formula for dose translation based on body surface area: Animal equivalent dose (mg/kg) = Human dose (mg/kg)/(Animal Km/Human Km) [12] ().
Hot plate test
Hyperalgesic reaction on the hot plate test is produced from a combination of the central and peripheral mechanism [13]. Noxious thermal stimulus was administered to rats by placing them on a hot plate analgesia meter (model 144-E52 Columbus, USA) maintained at 53 °C for 15 min before the experiment. Drugs were orally administered via oral gavage method for 1 week after four weeks of diabetes induction. The reaction time (hot-plate latency) was recorded. The reaction time was taken as the time between placing the rats on the hot plate and the time when they licked their paws. A cut-off time of 60 sec was used to prevent any thermal injury to the rats.
Statistical analysis
Results were expressed as mean ± SEM, and were analyzed by one-way analysis of variance (ANOVA). Significant differences between groups were determined by Dunnett test for multiple post-hoc comparisons using IBM SPSS Statistics 20 software. Statistical significance was accepted at p < 0.05.
Results
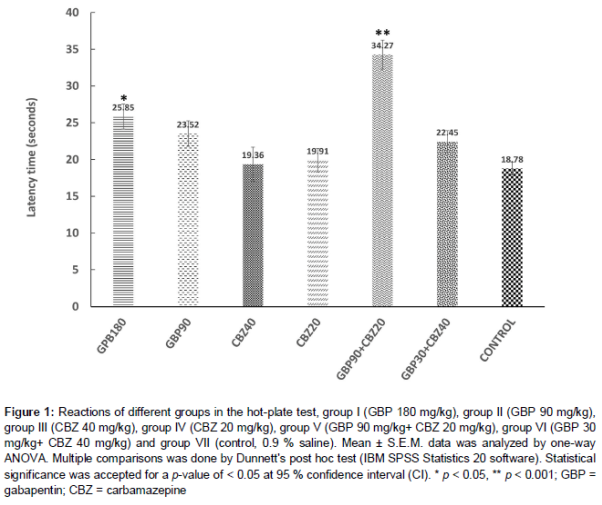
Analgesia
The analgesic effect of CBZ, GBP and their combinations on acute thermal nociception were tested using hot-plate test. Hot plate latencies significantly increased with oral administration of GBP at a dose of 180 mg/kg when compared with control group (p < 0.05), while at a dose of 90 mg/kg, the increase was not statistically significant. Oral administration of CBZ at doses of 20 and 40 mg/kg did not produce any significant effect on the hot plate latencies. However, combination of GBP at 90 mg/kg and CBZ at 20 mg/kg produced a significant increase in the hot plate latencies relative to the control group, and other groups (p < 0.05) except group I (GBP 180 mg/kg). The combination of GBP and CBZ at 30 mg/kg and 40 mg/kg, respectively caused slightly increases in hot plate latencies though this was not significant when compared to the other groups ().
Discussion
STZ is highly toxic for β-cells and is widely used to produce rodent models of type 1 diabetes. The progress of STZ induced diabetic neuropathy is primarily dependent on high glucose level, and on the duration of the high glucose level. In the early stage of diabetes in STZ rats, allodynia and hyperalgesia appeared to be induced during the first month of the onset of hyperglycemia in STZ rats [14]. Relative progression towards degenerative neuropathy is delayed in STZ-diabetic rats and at least transiently, they show indices of allodynia and hyperalgesia that make them a viable model for studying aspects of painful diabetic neuropathy [15].
The mechanism of neuropathic pain is manifested at two levels: the peripheral and central levels. On the peripheral level, there is an up-regulation of sodium channels in areas of axonal damage leading to decreased threshold and ectopic discharges. On the spinal level, there is an increased entry of calcium into the cell and potentiation of calcium-mediated effects [16].
CBZ appears to limit the repetitive firing of action potentials evoked by a sustained depolarization by reducing the rate of recovery of voltage-activated Na+ channels. At therapeutic doses, CBZ is selective in that there are no effects on spontaneous activity or responses to GABA or glutamate [7].
GBP acts by binding to the alpha-2-delta subunit of the calcium channel reducing neurotransmitter release. It is an antiepileptic drug with a structure similar to GABA, which is a neurotransmitter that plays a role in the pain mechanism [8]. GBP acts centrally to reduce hyperalgesia and allodynia, but it does not have significant actions as an anti-nociceptive agent [17]. In contrast, CBZ preferentially suppressed thermal nociception, due partly to the local anaesthetic action of sodium channel blocking agents, and differential sensitivities of the fibers activated by thermal nociception to local anaesthetic [18].
Previous clinical study has demonstrated absence of pharmacokinetic interactions between these combined therapies, along with the possibility of minimizing adverse effects, while significantly improving pain control in Trigeminal Neuralgia in Multiple Sclerosis [19]. No pharmacokinetic interaction exists between CBZ and GBP and dose adjustments are not necessary when GBP and CBZ are concurrently used [20].
Conclusion
The combination of GBP and CBZ in the hot-plate test at doses equivalent to human therapeutic doses of the two drugs was more efficacious than GBP and CBZ the drugs were given separately. Combining two medications with different mechanisms of action is a common strategy in the treatment of many medical disorders. The aim is to achieve a synergistic effect in the drug treatment, especially if there is no interaction between the drugs. The findings in this study provide additional data concerning combined treatment of pain in diabetic neuropathy with GBP and CBZ.
Declarations
Acknowledgement
References
Archives


News Updates